ICD-10 Code For Congestive Heart Failure I50.9 | Complete Guidelines
CHF is a clinical problem prevalent in clinical practice. It is a key factor in Medicare reimbursement and payer audit reviews. The use of the appropriate ICD 10 code for Congestive Heart Failure is now more than ever before, with millions of hospital admissions annually and billions spent on treatment.
The real challenge that healthcare providers face is accurate documentation. It is no longer enough to come to a general diagnosis. In order to make correct claims and risk adjustment, medical records should be absolutely specific on the type of heart failure that is being dealt with, be it diastolic, systolic, or a combination of the two.
An incorrect or incomplete ICD 10 code for Congestive Heart Failure may result in inaccurate reporting of data. Thus leading to claim denials and scrutiny of compliance, and further loss of much revenue.
After considering all the above details, the guide aims to assist in bridging the gap between clinical documentation and proper medical coding in clinics. which allows the healthcare organisation to enhance compliance, enhance the accuracy of claims, and maximise its revenue cycle.
Congestive Heart Failure and Its Symptoms
Congestive Heart Failure (CHF) is a chronic and progressive heart disease whereby the heart cannot pump blood effectively to satisfy the requirements of the body. From a medical billing and coding perspective, it is important to identify these clinical indicators to make the right assignment of the ICD 10 code for Congestive Heart Failure.
|
Symptom |
Clinical Presentation |
|
Dyspnea |
Shortness of breath (exertion or lying flat) |
|
Fatigue |
Constant exhaustion; low physical capacity |
|
Edema |
Pitting swelling in legs, ankles, and feet. |
|
Heart Rate |
Increased (tachycardia) or irregular pulse |
|
Congestion |
Persistent coughing or wheezing |
Documentation Gap
Healthcare providers should be more specific when documenting the condition in order to guarantee accurate coding and correct reimbursement. It should be clearly documented, both the nature of heart failure, e.g., diastolic, systolic, or mixed, and the acuity of the illness, e.g., acute, chronic, or acute-on-chronic.
Such a degree of classification enables coders to give the most suitable ICD-10 code and facilitate compliant and accurate claims submissions.
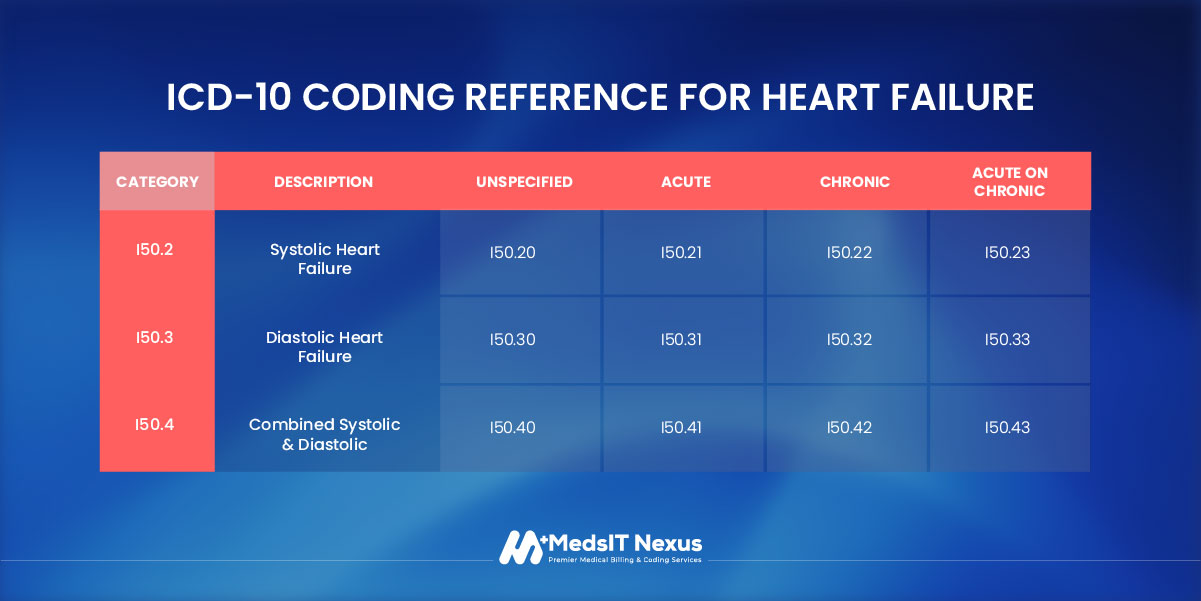
ICD-10 Coding Reference for Heart Failure
|
Category |
Description |
Unspecified |
Acute |
Chronic |
Acute on Chronic |
|
I50.2 |
Systolic Heart Failure |
I50.20 |
I50.21 |
I50.22 |
I50.23 |
|
I50.3 |
Diastolic Heart Failure |
I50.30 |
I50.31 |
I50.32 |
I50.33 |
|
I50.4 |
Combined Systolic & Diastolic |
I50.40 |
I50.41 |
I50.42 |
I50.43 |
Understanding Heart Failure ICD-10 classification
Heart failure icd 10 is classified within ICD-10-CM Chapter IX: Diseases of the Circulatory System (I00–I99). Within this chapter, CHF specifically falls under subcategory I50, which is designated for heart failure. This chapter encompasses a wide range of cardiovascular conditions, including ischemic heart disease, cardiac arrhythmias, and hypertensive heart disease.
When assigning codes, medical coders must carefully evaluate whether CHF is documented as a complication or result of another underlying condition, particularly hypertension. For example, if the provider documents hypertensive heart disease with heart failure, the appropriate code may include I11.0, along with an additional diagnosis code i50 9 code category to specify the type of heart failure.
In such situations, proper sequencing rules apply, and both the hypertension-related code and the specific CHF code may need to be reported to ensure accurate documentation and compliant billing.
CPT Codes for CHF Management
|
Service Category |
CPT Codes |
Description |
|
Initial Hospitalization |
99221–99223 |
Initial care for admitted CHF patients |
|
Subsequent Hospital Care |
99231–99233 |
Daily monitoring and treatment during stay |
|
Echocardiography |
93306 |
Complete heart function/severity assessment. |
|
Lab Collection |
36415 |
Venous blood draw (for BNP/NT-proBNP tests) |
|
Complex Care Add-on |
G2211 |
Medicare code for ongoing, complex CHF care |
CHF Management & Treatment Pathways
Congestive Heart Failure (CHF) management is usually a complex issue that is to be addressed with a combination of medication, medical equipment, and lifestyle modifications. From a revenue cycle management perspective, all treatments to be provided and should be properly recorded and correctly associated with the congestive heart failure coding guidelines.
Thus, this linkage helps determine medical necessity, facilitates billing compliance, and reduces the risk of payer denials.
Pharmacologic Management
Drugs are central to the treatment of CHF. To charge and document the clinical cases correctly, the providers are advised to document the reaction of the patient to the medication in the most accurate manner, especially at the time of the acute exacerbation or hospitalization.
Diuretics, including furosemide, are usually administered to assist in the reduction of fluid overload and alleviation of signs linked to congestion. Angiotensin receptor blockers (ARBs) and the ACE inhibitors are common medications to enhance heart performance and aid in enhanced blood flow.
Other critical aspects of the treatment are beta-blockers, which are useful in reducing the risk of complications and mortality in CHF patients. Aldosterone antagonists can also be incorporated in the treatment regimen in situations where the ejection fraction of the patient is also low, so as to supplement heart activity.
Pro Tips
In the case of intravenous diuretic Lasix used when hospitalizing a patient, it is necessary to make sure that the J1940 code is properly connected with the particular CHF diagnosis.
Moreover, the infusion services are to be reported with the help of the CPTs 9636596366 to fully reflect the process of the administration and ensure that the clinical resources spent in the course of the treatment may be paid in full.
Surgical Procedures and Device Therapy
Surgery or device-based treatments may be required in the presence of congestive heart failure (CHF) in more difficult situations, particularly when the patient has diastolic CHF or chronic systolic heart failure, ICD-10 with a significantly low ejection fraction. These measures are normally resorted to when the condition does not respond to medications and lifestyle modification.
One of them is the implantation of an implantable cardioverter-defibrillator (ICD). The ICD will avoid sudden death by identifying and treating dangerous arrhythmias. The CPT code used to bill the procedure is 33249. The abnormal heart rhythms and stable cardiac functioning can also be managed by pacemakers.
In more extreme cases, ventricular assist devices (VADs) are installed. VADs are artificial blood pressure assisting devices working as a provisional bridge to transplant or as a permanent, long-term destination therapy.
Compliance Note
These treatments are expensive; hence, payers have a close eye on them. The ejection fraction (EF) and New York Heart Association (NYHA) class of the patient must be clearly documented in clinical records. By ensuring the proper documentation, the procedure is justified according to the primary diagnosis of CHF by the ICD-10 and is compliant with the payer.
CHF Clinical Requirements
The proper ICD 10 Congestive Heart Failure (CHF) is determined by the thorough documentation of the provider. Coders are not permitted to rely on the labs or tests to make the diagnosis.
The notes should indicate the type as well as the acuity of the heart failure. Without such information, coders will be left to use an unspecified code, such as I50.9, which will put them at risk of payer audit, medical-necessity challenges, and claim rejection.
The Specificity Triple Threat
The documentation must address three main points to obtain the most accurate CHF ICD-10 code. The first step is to determine the nature of the heart failure: systolic (HFrEF), diastolic (HFpEF), or both. Second, characterize the acuity: acute episode, chronic condition, or acute on chronic heart failure icd 10.
Third, indicate the underlying cause, e.g., hypertension, ischemic cardiomyopathy, or valvular disease. The details include contributing to choosing the appropriate, compliant code by coders.
Checklist
|
Focus Area |
Key Documentation Elements |
Coding/Billing Impact |
|
Cardiac Function |
Document-specific Ejection Fraction |
Validates HFrEF vs. HFpEF |
|
Acuity Level |
Note exacerbation, decompensation, or overload |
Supports Acute/Chronic status |
|
Objective Data |
Include BNP/NT-proBNP and Echo results. |
Provides clinical validation for audits |
|
Radiology |
Note Kerley B lines or cephalization on X-ray. |
Evidence of pulmonary congestion |
|
Comorbidities |
Link CHF to Hypertension (Hypertensive Heart Disease) |
Shifts code to I11.0 (Higher RAF) |
Key Note
When the provider indicates CHF but the echo indicates a maintained ejection fraction (approximately 60 per cent), do not use the unspecified code automatically. Rather, request the provider to tell whether the patient has diastolic heart failure, so that the appropriate icd 10 code for diastolic heart failure I50.3 series can be used. This maintains coding correct, appropriate, and well reimbursed.
How to Avoid Claim Denials?
Claim denials related to icd 10 code for heart failure often occur due to incomplete documentation or inconsistencies between ICD-10 diagnosis codes and CPT procedure codes. Ensuring accurate and detailed clinical records is essential for supporting medical necessity, maintaining compliance, and preventing reimbursement issues.
-
Unspecified coding
-
Sequencing errors
-
Incomplete linkage
-
Risk adjustment validation
If the documentation lacks sufficient specificity or does not adequately support the diagnosis, the payer may deny the claim or remove the HCC credit. This can lead to lower patient risk scores and reduced reimbursement for the provider organization.
Denial Prevention Strategies
To minimize claim denials and improve reimbursement outcomes, providers should follow several best practices. Coding should always reflect the highest level of specificity supported by the clinical documentation.
If details in the medical record are unclear or incomplete, coders should query the provider for clarification before submitting the claim. It is also important to follow payer-specific coding guidelines, as requirements may vary among insurance plans.
FAQs
What is the ICD 10 code for congestive heart failure?
The ICD-10 code for congestive heart failure (CHF) is I50.9, Heart failure, unspecified.
Is I50.9 a billable ICD 10 code?
Yes, I50.9 ICD-10-CM code is a billable specific ICD-10-CM code that can be used for reimbursement and diagnosis reporting.
What does I50.9 mean in ICD 10?
In I50.9 ICD-10-CM code, I50.9 means heart failure, unspecified, indicating congestive heart failure without a specified type.
Why Should You Avoid Using I50.9 as the Primary ICD 10 Code for Congestive Heart Failure?
Using i50.9 icd 10 indicates that the clinical documentation lacks sufficient detail. Payers typically view unspecified codes as incomplete or inadequate documentation.
What Are the Sequencing Rules for CHF and Hypertension in ICD-10 Coding?
According to ICD-10-CM guidelines, hypertension and heart failure are often considered to have a causal relationship when documented together.
Which CPT Codes Should Be Linked to CHF ICD-10 Codes for Proper Billing?
To support reimbursement, CPT and HCPCS procedure codes should be directly linked to the relevant CHF diagnosis codes.
Table of Contents
Services
- Medical Audit Services
- Medical Billing Services
- Medical Credentialing Services
- Medical Coding Services
- Accounts Receivable Management
- Medical Insurance Verification
- Denial Menagement Services
Who we serve
- Private Practices
- Small Practices
- Hospitals & Healthcare
- Physicians
- Medical Equipment
- Outpatient Facilities
Get in Touch
Let's start talking about getting you credentialed